
Disease dilemmas (2026)
Viruses do not respect borders: cross-country cooperation remains crucial to global health.

[Welcome to the latest batch of new subscribers brought from Geoff Gibson’s Substack. Many of you will have seen that this has been rebranded as ‘The Bight’. So, to reciprocate, if new to it, have a look here. ]
Introduction
The past few weeks have brought unpleasant echoes of the Covid pandemic: mysterious deaths aboard a cruise ship, a virus that causes a deadly respiratory illness and talk of forced quarantines. Firstly, there was an outbreak of hantavirus followed by a rapidly escalating Ebola outbreak in central Africa, with hundreds of suspected cases and many deaths.
Neither of these outbreaks is likely to have the effect the coronavirus did. The hantavirus can cause severe illness and death, but it isn’t greatly contagious and tends to die out. The Ebola epidemic in the Democratic Republic of Congo (see below) is scarier, but even that is likely to stay confined to DRC and its immediate neighbours, according to the World Health Organisation (WHO).
In late May 2026 the annual meeting of WHO took place in Geneva, Switzerland, and began with a report suggesting that disease outbreaks are not only occurring more frequently, they are also becoming more damaging - and the world is increasingly struggling to fight and recover from them.
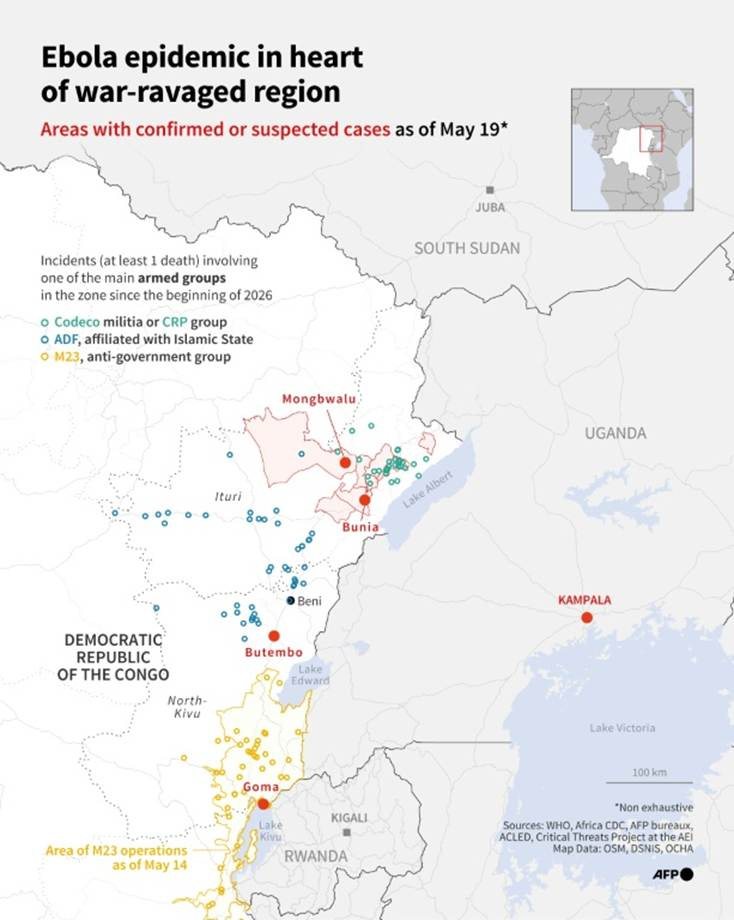
A health worker at a checkpoint near Goma (DRC).

Photo. The New York Times
Cooperation?
Recent years have highlighted that scientists have developed the ability to analyse new pathogens with speed and accuracy and to make new vaccines remarkably quickly. However, the legacy of Covid has divided the world. Richer countries have hung on to their vaccines, giving out booster doses to their citizens before many in poorer countries received their first dose. Within many countries, policies on lockdowns, school closures and vaccine mandates have created political rifts and deepened mistrust in scientists.
At the WHO meeting, there were discussions of a new pandemic treaty. Low-income countries have said they are willing to swiftly share genetic sequences and samples of emerging pathogens - but only in exchange for equitable access to the tests, vaccines and treatments that are developed with that information. Some developed countries have been unwilling to offer those guarantees. The USA did not attend the meeting.
The USA absence
A major blow to global health occurred when the Trump administration abruptly shut down the U.S. Agency for International Development (USAID) and ended most foreign aid, shifting instead to agreements with individual countries, often with strings attached. The administration also withdrew from the WHO and rejected a global framework that obligates countries to report outbreaks.
The impact of these decisions is becoming obvious. American officials were not among those investigating the hantavirus outbreak aboard the cruise ship, and they initiated their response nearly a month after the first death. They only learned of the new Ebola outbreak nine days after the WHO first alerted other global health authorities. The U.S. was once the undisputed leader in any outbreak. It coordinated the response, providing funding and expertise. The Ebola epidemic already suggests that the lack of American leadership highlights weaker surveillance of infectious diseases, delays in testing and a lack of crucial protective gear for health care workers on the front lines. In recent days, the US has stated that its own citizens who might have been in contact with Ebola should quarantine in Kenya, rather than be returned to, and isolated in, the USA.
Added to this, other countries, notably the UK and Germany, have also greatly reduced their international aid budgets, citing financial issues regarding increased levels of defence spending (resulting from pressure by the USA).
The Ebola outbreak 2026 (DRC)
The WHO declared a global health emergency due to an outbreak of Ebola virus in the Democratic Republic of the Congo (DRC) and Uganda in May 2026. The fast-spreading Bundibugyo variant of Ebola virus advanced rapidly in Ituri Province, a region of the DRC that borders Uganda and South Sudan. The WHO suspects that at least 200 deaths and 600 cases have been caused by the current outbreak. Without a vaccine, containment is the top priority, but a highly mobile population supporting the local gold mining industry, limited government control, ongoing armed conflict, mass displacement, and a humanitarian crisis marked by severe resource shortages all present challenges. Health workers and the communities they serve are trying to work in an extremely difficult situation for the case finding, contact tracing, and care-giving required to contain the outbreak (see map below).
The Ebola outbreak spreading across Democratic Republic of Congo and into neighbouring Uganda became an early test of what a retreat in Western health funding might mean for global pandemic preparedness. For years, the US financed networks of laboratories, epidemiologists and emergency-response programs through agencies including USAID and the Centres for Disease Control and Prevention. Those systems were designed not only to combat diseases such as HIV and malaria, but to identify dangerous pathogens before they spiralled into regional crises.
The Trump administration’s withdrawal of health funding that once helped support outbreak detection across parts of Africa represents the kind of cuts that contribute to the erosion of disease-surveillance systems. Health officials say the Bundibugyo strain of Ebola may have circulated undetected for six to eight weeks in northeastern Congo before lab testing confirmed the virus. By the time Ebola was identified, suspected cases and unexplained deaths had already spread across multiple health zones near the Ugandan border. The delayed detection is especially concerning because the Bundibugyo ebolavirus remains poorly understood compared with the Zaire strain responsible for the devastating West African epidemic a decade ago.
Footnote:
Yesterday, May 27th 2026, the International Rescue Committee (IRC) said the Ebola outbreak in the DRC is spreading faster than the response, as overcrowded camps for displaced people, poor conditions and limited supplies fuel fears the virus could spread further across the region. The IRC warned the outbreak could become the deadliest on record without urgent action.
That same day Uganda closed its border with the DRC after seven cases of the disease were confirmed in the capital Kampala.
Conclusion
Systems built with international aid often serve multiple purposes: tracking outbreaks, transporting laboratory samples and monitoring unexplained illnesses in remote regions. When funding disappears, those networks weaken quickly. The case of Ebola illustrates what happens when fragile surveillance systems face simultaneous pressure from conflict, donor fatigue and shrinking levels of international aid.
And, finally, a climate change-linked update….
The WHO has also warned that dangerous human-snake interactions could increase across the world as snakes migrate due to climate change. The ranges of highly venomous snake species such as cottonmouth moccasins in North America, kraits in Asia, and the black mamba in Africa could shift due to rising temperatures and human encroachment, bringing snakes closer to densely populated areas and places where venomous reptile species never lived before. Increased proximity could be deadliest in poorer, rural areas, where farmers often work the fields without shoes and healthcare is far away and not easily accessible.
Risks are also high for the snakes, with some species facing possible extinction. Coral snakes in the Amazon, puff adders in Africa, and copperheads in Papua New Guinea are threatened by both hotter weather and increased levels of conversions of wetland, grasslands, and forests into monoculture, cattle ranches, and towns.
Hiss…sss.